
A preclinical model that captures the full complexity of CKM syndrome
Cardiovascular–kidney–metabolic (CKM) syndrome is increasingly recognised as asystemic condition yet preclinical research still tends to treat heart, kidney andmetabolism as separate domains. A new TNO-developed mouse model brings thesesystems together, opening the door to more realistic and translationally relevantresearch.
CKM syndrome: a systemic problem, still studied in fragments
Obesity, type 2 diabetes, chronic kidney disease and cardiovascular dysfunction rarely occur in isolation. In patients, these conditions interact and reinforce one another and accelerate disease progression. This interconnected pathology is now recognised as cardiovascular–kidney–metabolic (CKM) syndrome formally defined as a distinct clinical entity by the American Heart Association in 2023.
Despite this recognition, most preclinical models continue to focus on a single organ or pathway. Promising therapies regularly fail to translate from bench to bedside, not because they lack biological effect, but because they are tested outside the systemic context in which CKM syndrome actually unfolds.
Building a model that mirrors real disease progression
To address this gap, TNO researchers together with both academic and industry partners developed a multifactorial diet-induced mouse model designed to capture the progressive interplay between metabolic dysfunction, kidney failure and cardiac remodelling.
The model combines the KK-Ay genetic background, which results in spontaneous development of obesity and type 2 diabetes, with uninephrectomy, a high-fat diet and L-NNA-induced hypertension. This combination reproduces key clinical features seen in CKM patients: obesity, hyperglycaemia, progressive diabetic and chronic kidney disease, and cardiac dysfunction consistent with heart failure with preserved ejection fraction (HFpEF).
Importantly, disease progression emerges from the interaction of multiple stressors rather than from isolated genetic manipulation, which substantially increases its translational relevance.
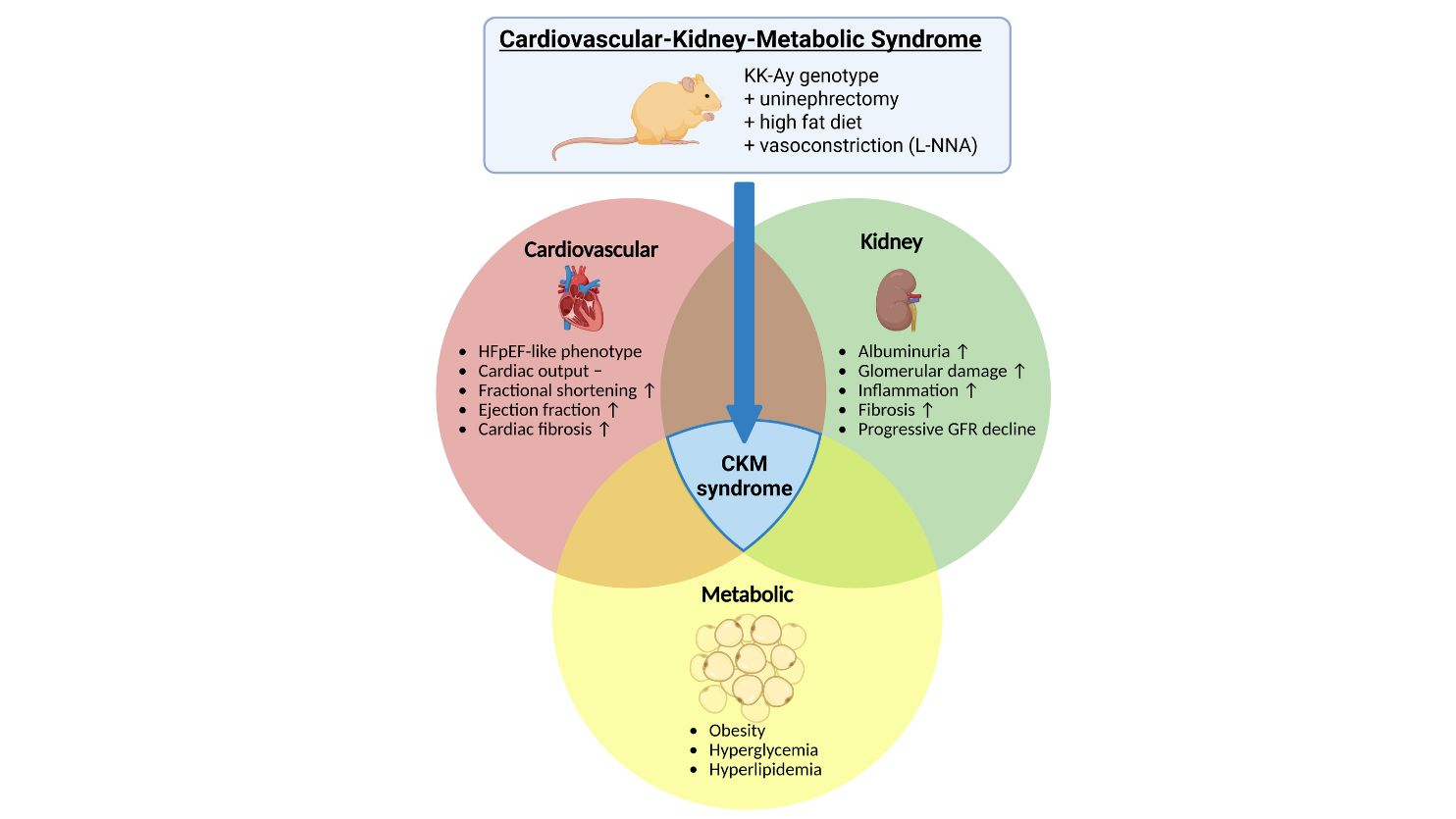
One of the most striking aspects of the model is its renal phenotype. The mice develop early albuminuria and transient hyperfiltration, followed by a sustained and progressive decline in glomerular filtration rate (GFR), thereby closely mirroring the disease trajectory observed in patients with diabetic kidney disease. In a 20-week follow-up study, GFR declined by 44% from peak hyperfiltration, meeting established criteria for clinically meaningful CKD progression.
Histological analysis revealed pronounced glomerulosclerosis, tubulo-interstitial fibrosis and inflammation, with glomerular basement membrane thickening and arteriolar hyalinosis characteristic of advanced diabetic kidney disease. Transcriptomic profiling of renal tissue further confirms robust activation of inflammatory and fibrotic signalling pathways, including upstream regulators such as TGFB1, NFκB and IL-1β alongside suppression of mitochondrial biogenesis, reflecting mechanisms increasingly identified as key drivers of CKD progression in humans.
Beyond the kidneys, the model also captures meaningful cardiac involvement. Functional measurements show increased ejection fraction and fractional shortening alongside concentric left ventricular remodelling, changes consistent with a compensatory hypertrophic response rather than true systolic improvement. Histologically, pronounced right ventricular fibrosis is present, most markedly at the septal insertion points. Together, this pattern points towards an HFpEF-like phenotype.
HFpEF is one of the most heterogeneous and therapeutically challenging forms of heart failure, and its association with metabolic and renal disease is well established but poorly modelled preclinically. The ability to study cardiac remodelling alongside progressive kidney disease and metabolic dysregulation within a single experimental framework is a meaningful step forward.
From mechanism to medicine: testing therapies in context
The strength of this CKM model lies not only in its biological realism, but in its applicability as a platform for therapeutic research. The model is being developed as a shared framework within which interventions can be evaluated across metabolic, renal and cardiac endpoints simultaneously.
Early findings from the model also have mechanistic implications for treatment strategy: the data show that L-NNA-induced hypertension substantially accelerates both renal decline and cardiac remodelling on top of the metabolic disease burden, raising important questions about the timing and cardiovascular consequences of blood pressure management in CKM syndrome.

'CKM syndrome is not a collection of separate diseases, it is a systemic process, If we want therapies that work in patients, we need models that reflect that reality.'
A platform for collaboration and translational alignment
At TNO, preclinical models are developed with implementation in mind. This CKM model functions as a shared research platform where academia, industry and healthcare stakeholders can align on disease mechanisms, study endpoints and translational strategies.
Besides optimising for a single outcome in one organ of interest, the model also allows researchers to assess whether interventions meaningfully alter disease trajectories across organ systems. This supports more informed go/no-go decisions in drug development, and focuses resources on therapies with genuine system-level impact.
Standard-of-care medication including the SGLT2-inhibitor Dapagliflozin and GLP1-receptor agonist Semaglutide were effectively tested in this model and capable of reduced both the metabolic burden as well as preventing the strong decline in renal function and damage.
Looking ahead
As the global burden of CKM syndrome continues to rise, the need for integrated, multifactorial research approaches becomes increasingly urgent. Future work will focus on expanding therapeutic testing across treatment classes, refining early-intervention strategies and biomarkers and identifying which disease features are reversible and at what stage.
More broadly, this model illustrates a shift in biomedical research: from isolated targets towards system-level understanding, where translational relevance and cross-disciplinary collaboration determine impact.
Interested in using this CKM model for translational research or therapeutic testing? Contact TNO to explore collaboration opportunities.
Contact us
-

Arianne van Koppen
Functie:Scientist Health & Work-
Standplaats:Leiden - Sylviusweg
-
Email:Email Arianne
-
Get inspired
14C-Pulse-Chase Technology

Obesity
Diabetic kidney disease

MASH and liver fibrosis

HistoSuite: AI-powered histopathology